

Imagine you are having lunch with friends when suddenly your throat tightens, your skin breaks out in hives, and breathing becomes difficult. In those seconds, time slows down, and one decision could save your life. This terrifying scenario describes anaphylaxisa severe systemic hypersensitivity reaction characterized by rapid onset that may cause death if untreated, originating from Greek roots meaning "without protection" and clinically described in 1902. It is not just a bad rash or a tummy ache; it is a full-body medical emergency that requires immediate action. While many people know they are allergic to peanuts or bees, recognizing when an allergy turns deadly is often the hardest part. Understanding the signs and the right tool can mean the difference between walking away and needing hospital care.
The Reality of Severe Allergic Reactions
Every year, millions of people face sudden reactions to things their immune system mistakenly identifies as threats. Current data suggests approximately 1.6% of the US population has experienced this event, translating to over 5 million individuals living with this risk. These reactions don't wait for convenience. They can happen anywhere-schools, offices, or family gatherings. The triggers vary widely. Foods remain the biggest culprit, with peanuts, tree nuts, and shellfish accounting for 90% of food-induced cases. Insect stings, specifically from Hymenoptera venom like honeybees and wasps, are responsible for nearly 10% of cases seen in emergency departments. Even medications we trust, such as penicillin, can trigger severe responses in susceptible people.
The body's response is aggressive. When the immune system sounds the alarm, it releases histamine and other chemicals that attack multiple systems simultaneously. You aren't just dealing with one symptom; you are often dealing with a cascade failure. Skin symptoms like urticaria (hives) appear in 80-90% of cases, making them the most visible sign. However, relying on hives alone is dangerous. Airway issues occur in 70% of incidents, manifesting as wheezing or stridor. More insidiously, cardiovascular problems like hypotension (low blood pressure) affect about 35% of victims. Without intervention, the progression is fast, with fatality rates ranging from 0.3% to 1% in retrospective studies.
Why Epinephrine Is the Gold Standard
If you have ever heard someone say, "Just give him some Benadryl," stop them immediately. Antihistamines like diphenhydramine have been shown to have 0% efficacy as a standalone treatment for this condition. Similarly, corticosteroids show no benefit in acute management, though they might help prevent a second wave of symptoms later. The only medication proven to reverse the life-threatening changes is epinephrinea hormone that counteracts airway compromise, respiratory distress, and circulatory collapse through alpha-adrenergic receptor-mediated vasoconstriction. It works by tightening blood vessels to raise blood pressure and opening airways to restore breathing. Expert consensus identifies this drug as the cornerstone of management, with leading specialists stating there is simply no substitute.
The timing of this administration is critical. Guidelines from the Resuscitation Council UK (2021) specify that treatment should begin at the first sign of severity. Waiting is the single greatest predictor of poor outcomes. In fact, studies indicate that 85% of patients improve within 5 minutes of receiving the shot, compared to only 42% with delayed administration. Intramuscular injection achieves therapeutic plasma levels 3 to 5 times faster than intravenous methods in non-arrest settings. The standard dosing involves 0.3 mg for adults and adolescents weighing over 30 kg, while children between 15-30 kg receive 0.15 mg. This precision ensures the drug hits the bloodstream quickly enough to stop the reaction before organ damage occurs.
Mastering the Auto-Injector Device
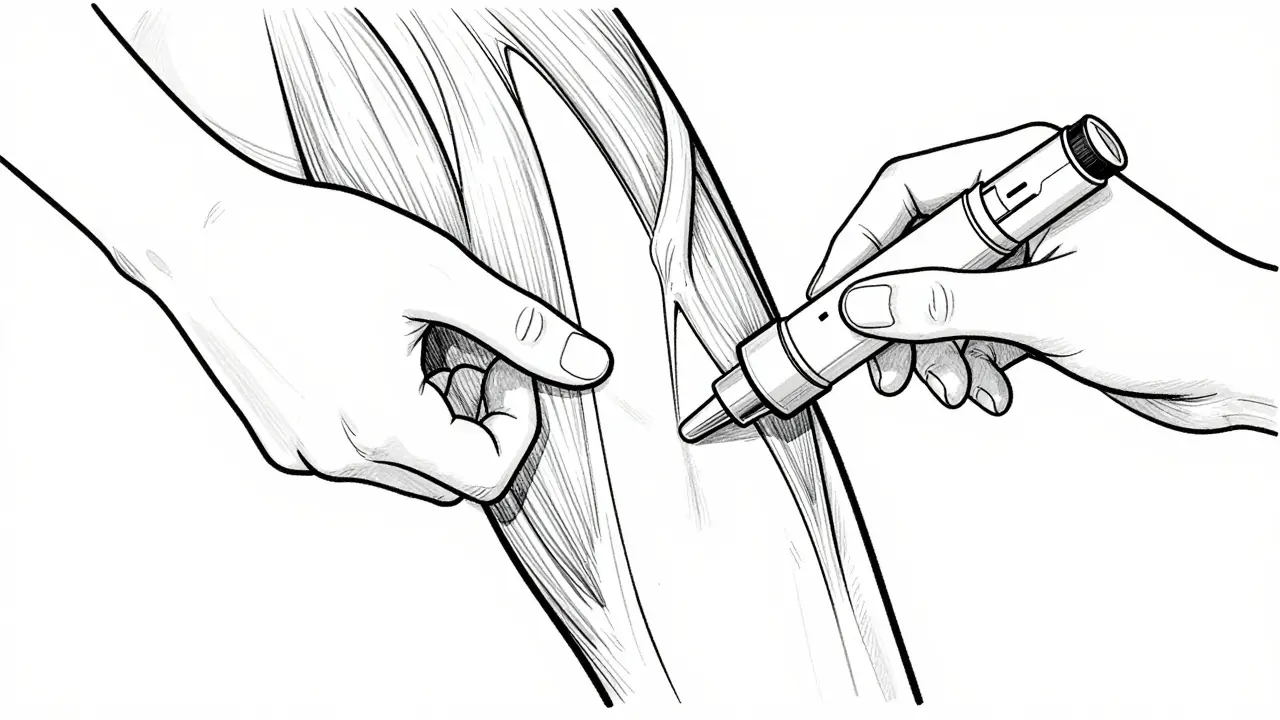
In real-world situations, doctors aren't always present. This is where the auto-injector becomes essential. Market positioning shows devices like EpiPen, Auvi-Q, and Adrenaclick are the primary tools available. The EpiPen historically dominated the market, holding 85% share in 2016, but competition has increased with voice-guided systems like Auvi-Q. Regardless of the brand, the goal remains the same: delivering the medicine into the thigh muscle. The anterolateral thigh (vastus lateralis muscle) is the target site because it allows for rapid absorption. Peak plasma concentrations occur in about 8 minutes via intramuscular injection, compared to 20 minutes if injected subcutaneously.
Using the device correctly requires practice. Research indicates that 68% of users demonstrate incorrect technique during simulated emergencies. Common errors include removing the cap with too much force, failing to hold the device in place long enough, or injecting into the buttocks or arm instead of the thigh. Proper technique involves pressing the device firmly against the outer thigh until it clicks, holding it for three seconds, and then massaging the area. Training takes about 20-30 minutes to master initially, but regular practice keeps skills sharp. Many experts recommend practicing with trainer devices monthly to avoid anxiety during actual crises.
| Treatment Option | Effectiveness | Time to Onset | Recommended Use |
|---|---|---|---|
| Epinephrine | High (First-Line) | Minutes | Immediate Acute Emergency |
| Antihistamines | Low / None for Shock | 30+ Minutes | Adjunctive (Skin Symptoms Only) |
| Corticosteroids | None for Acute Phase | Hours | Prevent Biphasic Reactions |
Storage, Expiry, and Maintenance
Owning the device is useless if it doesn't work when pulled out. Auto-injectors have a shelf life, typically lasting 12 to 18 months. Storing them correctly is vital for maintaining potency. Room temperature between 20-25°C (68-77°F) is ideal. Avoid leaving them in hot cars or freezing environments, as extreme temperatures degrade the medication quality. A common pitfall is keeping expired units in emergency bags. Setting a reminder app notification six months before expiration ensures you replace the device in time. Recent industry developments include extended-shelf-life formulations currently in trials, which aim to solve the frequent replacement issue.
Financial barriers can also impact readiness. The cost of these devices varies significantly. As of 2023, list prices ranged from $375 to $650 per two-pack, though actual patient costs depend on insurance. This limits access for 30% of prescribed patients. Fortunately, generic alternatives now cover 70% of prescriptions in some markets, bringing average out-of-pocket payments down from $325 in 2016 to $185 in 2023. If cost is a concern, discussing pharmacy assistance programs with your provider is a necessary step to ensure you always have access to the treatment.
What Happens After the Shot?
Administering the dose isn't the end of the process. Immediate activation of emergency services (911 in the US, 000 in Australia) is mandatory regardless of how much better the person feels. About 20% of patients experience biphasic reactions, where symptoms return hours later without a new exposure. Because of this, high-risk patients-including those with asthma or cardiovascular disease-require observation periods of up to 12 hours. The 2021 Resuscitation Council UK guidelines mandate this observation window for anyone requiring multiple doses. During this time, medical teams monitor for recurrence.
Education extends beyond the victim. Schools are increasingly required to stock these devices, with 92% of US schools having mandated stock by 2022. Community awareness helps reduce the stigma around carrying these devices. Parents of food-allergic children show higher adherence rates (82%) compared to adults with insect allergies (54%). Encouraging family members and close friends to learn recognition signs creates a safety net. Remember, a delay of even 15 minutes can change the outcome, so acting fast is better than waiting for confirmation.

Emerging Technologies and Future Outlook
Innovation continues to evolve to support patients better. Telemedicine platforms now offer real-time support during an incident, guiding users through visual checks. New delivery methods, such as nasal spray epinephrine approved in late 2023, provide needle-free options for those with severe needle phobia. Smart injectors with Bluetooth connectivity are in prototype stages, capable of alerting emergency contacts automatically when used. Despite these advancements, the underlying physiology doesn't change. Omalizumab (Xolair) shows promise for high-risk patients, potentially reducing the need for shots by 67% in specific trials, but it is preventative rather than acute treatment.
Long-term viability assessments confirm that this hormone will remain first-line for the foreseeable future. Its unmatched efficacy profile makes it irreplaceable. However, persistent challenges remain regarding public knowledge gaps; 58% of adults cannot identify symptoms according to national surveys. Bridging this gap requires clear, accessible education on recognizing early warning signs. By prioritizing preparation and dispelling myths about milder treatments, communities can significantly reduce the fatality rate associated with these unpredictable events.
Frequently Asked Questions
Can I use an antihistamine instead of epinephrine?
No. Antihistamines like Benadryl are ineffective for stopping severe shock. Systematic reviews show they have 0% efficacy as monotherapy for this condition. Epinephrine is the only medication proven to reverse life-threatening symptoms rapidly.
How long does an auto-injector last?
Most devices have a shelf life of 12 to 18 months. You should check the expiration date regularly and store them at room temperature away from direct heat to ensure they function correctly when needed.
Where is the best place to inject?
The outer thigh (vastus lateralis muscle) is the recommended site. Injecting here provides the fastest absorption. Do not inject into buttocks, arms, or veins.
Do I need to go to the hospital after using the device?
Yes. Always call emergency services immediately after administration. Symptoms can return hours later (biphasic reaction), and medical monitoring for up to 12 hours is often required for safety.
What are the main symptoms to watch for?
Look for trouble breathing, swelling of the tongue/throat, widespread hives, or a sudden drop in energy/pressure. If these occur shortly after exposure to an allergen, treat it as a medical emergency.














8 Comments