
Shoulder pain doesn’t just happen out of nowhere. If you’ve been struggling with a dull ache that gets worse when you lift your arm, reach for a shelf, or try to sleep on your side - you’re not alone. About 2 million Americans see a doctor for shoulder pain every year, and most of it comes down to two closely linked problems: rotator cuff injuries and inflammation of the subacromial bursa, known as shoulder bursitis. These aren’t just minor annoyances. Left unchecked, they can stop you from working, playing sports, or even putting on a shirt. The good news? Most cases get better without surgery - if you know what to do.
What’s Actually Going On in Your Shoulder?
Your shoulder is a ball-and-socket joint, but unlike your hip, it’s not locked in place. It’s held together by muscles and tendons - especially the rotator cuff, a group of four small muscles: supraspinatus, infraspinatus, teres minor, and subscapularis. These muscles keep the ball of your arm bone centered in the socket while you move your arm. Overhead motions - like throwing, painting, or lifting boxes - put constant stress on them.
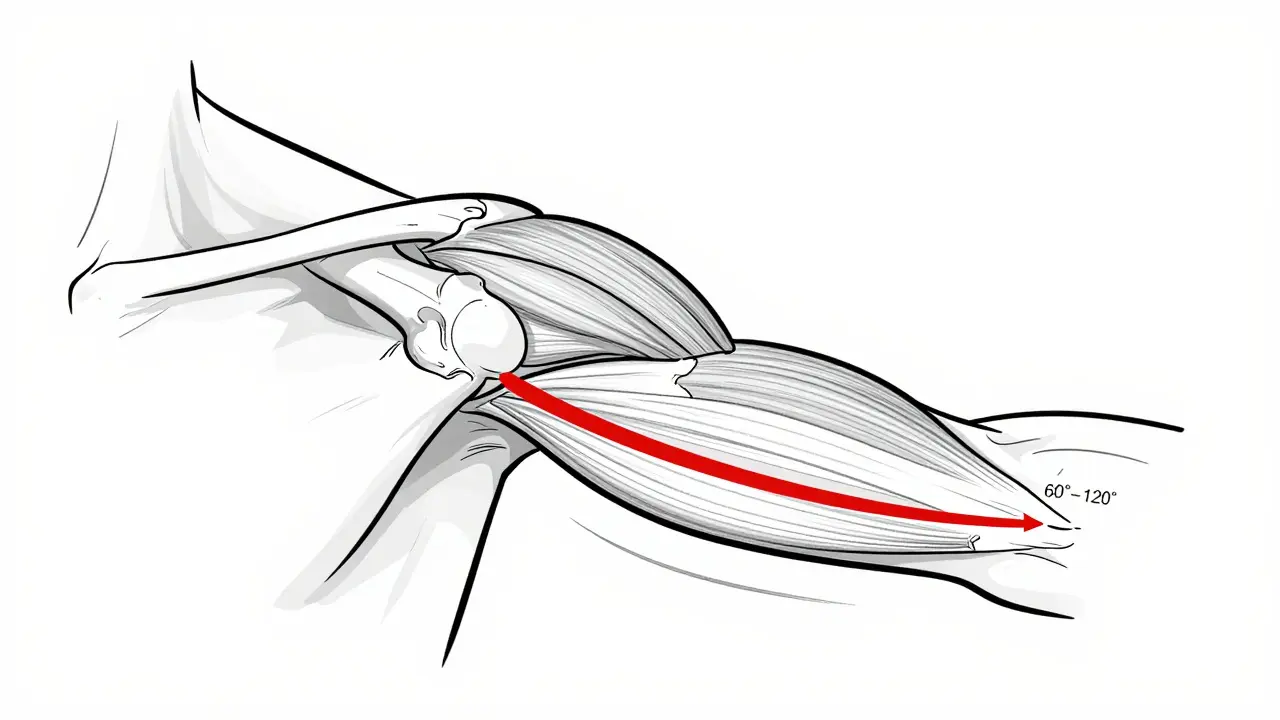
Right above these tendons sits a fluid-filled sac called the subacromial bursa. Its job? To reduce friction between the tendons and the bony roof of your shoulder (the acromion). When the bursa gets irritated, it swells up - sometimes to three times its normal size. That swelling pushes against the tendons every time you lift your arm. That’s impingement. And that’s where the pain comes from.
The classic sign? A painful arc. When you raise your arm sideways, it doesn’t hurt at first. Then, between 60° and 120°, boom - sharp or deep ache. After that, it eases again. That’s textbook impingement. Night pain is another red flag. If you wake up because your shoulder feels like it’s throbbing, especially when you lie on it, that’s a strong clue you’re dealing with bursitis or tendon inflammation.
Who’s Most at Risk?
This isn’t just an older person’s problem. While over 50% of people over 80 have some degree of rotator cuff wear, it’s not just about age. Think about your job or hobbies. Construction workers have a 32% higher chance of shoulder issues than the general population. Painters, electricians, swimmers, tennis players, and even people who carry heavy bags on one shoulder are all at risk. The real kicker? It’s not always one big injury. Most cases build up slowly from repeated small stresses - like typing with your arm raised, doing too many push-ups, or sleeping with your arm under your body for years.
And here’s something many don’t realize: you can have a torn rotator cuff and feel no pain at all. Studies show that 30% of people over 60 with full-thickness tears on MRI never had symptoms. That means pain doesn’t always equal damage. It’s more about how your shoulder is moving - and how much inflammation is around it.
What Should You Do First? (The Real Protocol)
If you’re in pain, your first instinct might be to rest completely. But that’s not the best move. The goal isn’t to stop movement - it’s to stop the irritating movement.
Here’s what actually works, based on clinical guidelines from the American Academy of Orthopaedic Surgeons and real-world data from top rehab centers:
- Stop the aggravators. Avoid lifting anything above shoulder height. Don’t sleep on the painful side. Skip overhead activities like reaching for cabinets or doing pull-ups. This isn’t about being lazy - it’s about giving the inflamed area a chance to calm down.
- Ice it. Use an ice pack for 15-20 minutes, 3-4 times a day. Don’t wrap it in a towel - direct contact works better. Cold reduces swelling and numbs the pain. Do this for the first 48-72 hours, then cut back to once or twice daily.
- NSAIDs help - but don’t overdo it. Ibuprofen (400-600 mg) three times a day for up to 10 days can cut inflammation. But if you’re taking it longer than two weeks, talk to your doctor. Long-term use can mess with your stomach and kidneys.
- Start moving - gently. Within 48 hours, begin pendulum exercises. Lean over a table, let your arm hang down, and swing it in small circles - 5-10 minutes, 3 times a day. This keeps the joint lubricated without stressing the tendons.
Most people feel better in 2-4 weeks just doing this. If not, it’s time to level up.
Physical Therapy: The Real Game-Changer
Here’s where most people give up - and where the real recovery begins.
Physical therapy isn’t just “do these three exercises.” It’s about fixing the whole system. Your shoulder doesn’t work alone. It’s connected to your neck, upper back, and even your posture. If your shoulder blades aren’t moving right, your rotator cuff is working overtime.
Effective rehab has three phases:
- Restore motion. After pain eases (usually in 2-3 weeks), start active-assisted stretches. Use your good arm to gently lift the painful one. Hold each stretch for 30 seconds, repeat 3 times, twice a day.
- Strengthen the scapula. This is the secret weapon. Most people focus only on the rotator cuff, but scapular stabilization is what actually takes pressure off the tendons. Do this daily: sit or stand tall, squeeze your shoulder blades together like you’re holding a pencil between them, hold for 5 seconds, release. Do 3 sets of 15. People who do this consistently recover 30% faster.
- Build rotator cuff strength. After 4-6 weeks, start using resistance bands. Attach the band to a doorknob, hold it with your elbow bent at 90°, and slowly rotate your arm outward (external rotation) and inward (internal rotation). Do 2-3 sets of 15 reps, 3-4 times a week. Keep the resistance light - 30-50% of your max. No pain, just control.
Studies show that patients who stick to this for 8-12 weeks have an 80% success rate. The key? Consistency. Not intensity. One study found that people using smartphone apps to track daily exercises completed 82% of their routines - compared to just 54% without reminders.
When Injections Make Sense (And When They Don’t)
If pain lingers after 6 weeks of rehab, corticosteroid injections are the next step. They’re not magic. They’re a reset button.
Under ultrasound guidance, a doctor injects a mix of steroid (like triamcinolone) and numbing medicine directly into the space between the bursa and the bone. It reduces swelling fast. About 70% of people get relief for 4-12 weeks. But here’s the catch:
- Don’t get more than 2-3 injections a year. More than that raises your risk of tendon rupture by 8%.
- It’s not a cure. It’s a window of opportunity. Use those 6-8 weeks to get serious about rehab.
- It doesn’t work for everyone. If you’ve had two failed injections, it’s time to rethink your approach - not get a third.
And here’s a newer option: platelet-rich plasma (PRP) injections. Approved in 2024 as a second-line treatment after steroids, PRP uses your own blood to trigger healing. One multi-center trial showed a 68% success rate - better than repeat steroid shots. It’s not covered by all insurance yet, but it’s gaining traction.
Surgery: What’s Really Necessary?
Surgery sounds scary - and it is. But only if you don’t need it.
Most shoulder surgeries for bursitis or tendinitis are arthroscopic. That means tiny incisions, a camera, and a small tool to shave down the acromion bone and remove the inflamed bursa. It takes about an hour. Recovery? 4-6 months with restrictions.
But here’s the hard truth: a 2022 study in the Journal of Bone and Joint Surgery found no real difference in outcomes between people who had surgery and those who did 6 months of physical therapy. If you don’t have a full-thickness tear, surgery doesn’t offer much advantage.
It’s only recommended if:
- You’ve tried 3-6 months of rehab and injections with no improvement.
- You have a complete rotator cuff tear - especially if you’re over 60 and need to use your arm for daily tasks.
- Your job or lifestyle demands overhead strength (e.g., carpenter, swimmer, firefighter).
And if you’re thinking about surgery, ask this: Do I have pain because of damage - or because I’m moving wrong? If it’s the latter, surgery won’t fix it.
What Really Works: Real Stories
A 54-year-old carpenter in Sydney stopped working after 3 months of shoulder pain. He tried ice, rest, and one injection. No luck. Then he started daily scapular exercises and pendulum swings. At week 12, he returned to work - full duty. No surgery.
A 37-year-old tennis player had tendinitis after a tournament. She added daily cryotherapy (ice massage) and eccentric strengthening (slow lowering of resistance) and was back in 10 weeks.
And the flip side? The “weekend warrior.” A guy who played basketball on Saturdays, ignored pain all week, then expected to be fine. He had three flare-ups in 8 months. He didn’t need surgery. He needed consistency.
What to Avoid
- Stretching too hard. Forcing your arm into painful positions makes inflammation worse.
- Using heat too early. Heat feels good, but it increases swelling in the first 2-3 weeks. Save it for after inflammation calms down.
- Ignoring night pain. If you’re waking up, your shoulder isn’t healing. Adjust your sleep position - try a pillow between your arm and body.
- Waiting too long. If pain lasts more than 6 weeks, don’t hope it’ll go away. See a physical therapist.
Final Thought: It’s Not About Strength - It’s About Control
Shoulder pain isn’t about being weak. It’s about being unbalanced. Your body isn’t broken. It’s just out of sync. The fix isn’t surgery, not even injections - it’s daily movement, smart pacing, and patience.
You don’t need to do 100 reps. You need to do 10 reps - correctly - every day. That’s how you rebuild.
Can shoulder bursitis heal on its own?
Yes - but only if you stop the actions that caused it. Resting alone isn’t enough. You need to change how you move, lift, and sleep. Most people who avoid overhead activity and do gentle daily mobility exercises see improvement in 4-8 weeks. But if you keep doing the same things, the inflammation will just come back.
Is heat or ice better for shoulder pain?
Ice is better in the first 3-7 days, especially if the pain is sharp or swelling is present. Use ice for 15-20 minutes, 3-4 times a day. After inflammation eases, you can use heat to relax tight muscles - but only if you’re doing exercises. Never use heat if you’re still in the acute pain phase.
How long does physical therapy take for shoulder bursitis?
Most people start feeling better in 4-6 weeks, but full recovery takes 8-12 weeks of consistent effort. The key is not how many sessions you go to - it’s how often you do the exercises at home. Daily scapular and rotator cuff work matters more than weekly therapy visits.
Can I still work out with shoulder bursitis?
Yes - but not the way you used to. Avoid overhead presses, pull-ups, bench presses, and swimming. Focus on lower body workouts and light cardio. Once pain eases, you can slowly reintroduce shoulder exercises - starting with pendulums and scapular squeezes. Never push into pain.
Do I need an MRI for shoulder pain?
Not usually. Most shoulder pain from bursitis or tendinitis can be diagnosed with a physical exam and history. MRIs are only needed if you’ve tried 3-6 months of rehab with no improvement, or if you suspect a full-thickness tear - especially if you’re over 60 or have sudden weakness. Imaging doesn’t change treatment for most cases.
Why does shoulder pain get worse at night?
When you lie down, gravity no longer helps reduce pressure on the inflamed bursa. Plus, your body’s natural anti-inflammatory chemicals are lower at night. Lying on the affected side compresses the area even more. Try sleeping on your back with a pillow under the painful arm, or on the opposite side with a pillow hugged to your chest.
Next Steps
If you’re still in pain after 6 weeks of consistent rehab:
- See a physical therapist who specializes in shoulders - not general rehab.
- Ask about ultrasound-guided injections if you haven’t had one.
- Consider PRP if steroids didn’t work.
- Don’t rush into surgery. Ask: Have I done everything non-surgical?
The shoulder is resilient. It just needs the right kind of care - not more force, not more drugs, not more cuts. Just smart, consistent movement.

















15 Comments